Technical Trends in Remote Patient Monitoring
Technical Trends in Remote Patient Monitoring: by Kieran Gonsalves, former Telecommunication and Mobile Computing Leader
I received an invitation to share my 30+ years of experience in Telecommunications and Mobile Computing with an audience of physicians, all far more knowledgeable in their respective fields than me. Apparently, in COVID times, the use of remote technology in delivering health services had suddenly become mainstream opening a Pandora’s box.
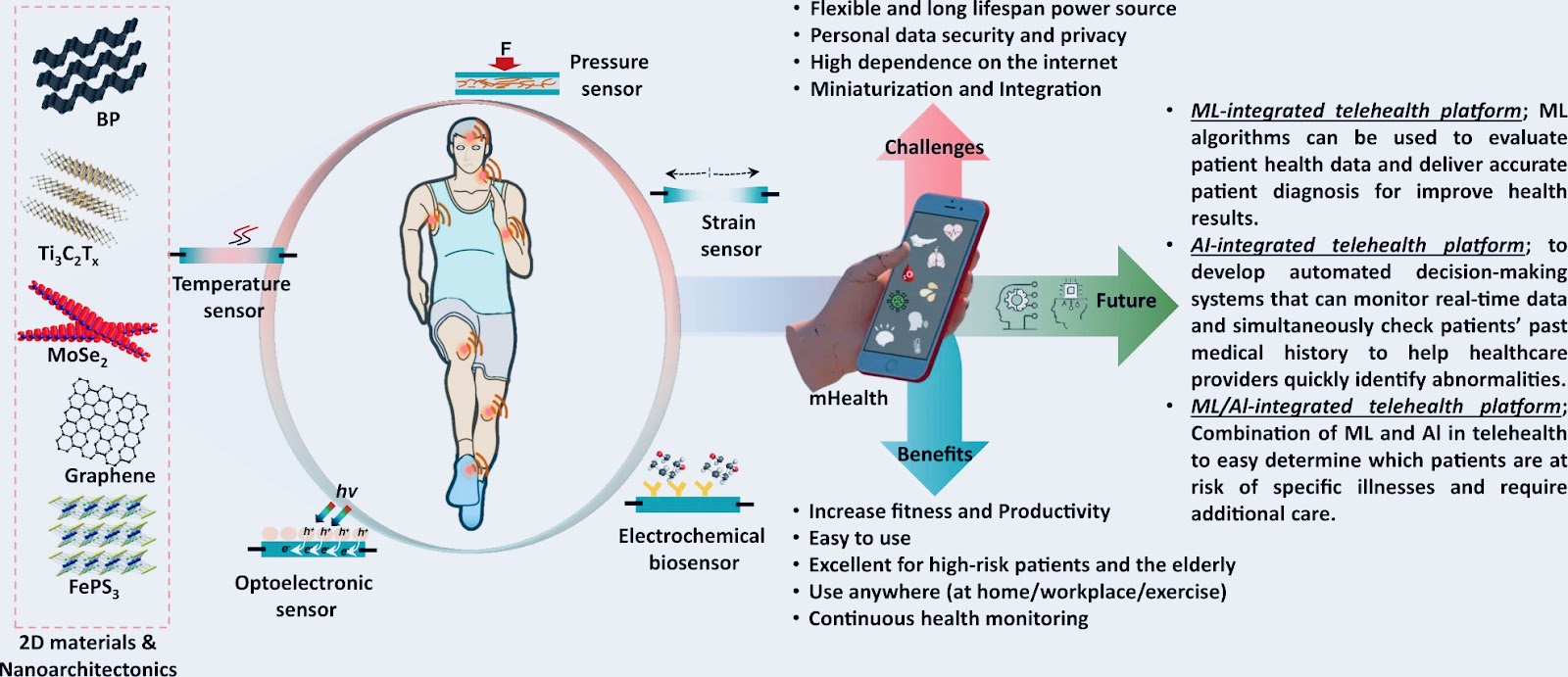
Source: Nature [3]
Now that I got you all puffed up, let me burst your bubble … the commoditization (read affordability and ubiquity) of mobile computing coupled with the rapid miniaturization of precision electronic sensors opened the floodgates of mRPM (mobile remote patient monitoring), which then exploded with the onset of the pandemic when face-to-face contact with the healthcare provider was not possible. Suddenly nurses and physicians' assistants rushed to deploy mRPM devices merely on promises - the health, safety and reliability standards would just have to wait till normal times returned they rationalised. Like things would ever get normal again 🙄!
Without clear Government oversight or Industry standards, a plethora of devices hit the market all with the promise of monitoring patients and painlessly escalating when a concerning trend requires the physician’s attention.
For those who were justifiably sceptical, a proverbial carrot in the form of big data analysis, AI and machine learning was dangled, promising to automate most of the repetitive tasks of healthcare givers so that they can use their precious time where it is actually needed the most.

Here are two such examples:
Dutch investigators have demonstrated that a smartwatch can be programmed to help evaluate and monitor motor functioning among patients with the disease. Their virtual motor exam required patients to perform a set of tasks, including raising and twisting their arms and getting up from a chair, which were recorded by the smartphone they wore on their wrist. The data helped clinicians evaluate several clinically essential signs, including rest tremor, bradykinesia, and arm swing during gait, enabling them to judge disease severity and response to medication.[1]
A 2022 report in the journal Nature described a thin strip of removal material embedded with tiny sensors to painlessly and automatically measure blood pressure. You stick it just above the wrist and go about your day normally, not even thinking about it. You can even exercise, including doing push-ups: the tiny sensors keep recording your pressure. Then, using your smartphone or smartwatch, and with your permission, the data can be automatically sent the the Internet to your healthcare provider’s office. Likewise, diabetes patients no longer need to prick their fingers to determine their blood sugar levels; they now can place their smartphone next to a little device pasted to their skin. [1]
Let’s talk about the elephant in the room - the long-term impracticality of rushing to mRPM market.
Let me give you a view through my Engineering lens, as I sometimes find myself doing when mentoring millennials, and I welcome hearing your concerns, as you, Physicians see.

For starters, patients value ease of use, low cost (affordability) and reliability. Let’s take a closer look at these
Ease-of-use: The most impactful trend seems to build health monitoring functionality into common consumer devices like the AppleWatch with its one-lead Atrial Fibrillation Diagnosis. In this way, we remove the social stigma that comes with wearing specialized consumer medical devices betraying a health problem. With time we slowly scale up the device’s capability, for example, by interacting with Blipcare Wi-Fi Weight Scale to monitor weight fluctuations which can detect rapid fluid retention a precursor to heart failure.
It goes without saying that, no special training or experience is needed to wear or use a watch. Clinical on-body medical devices are of course the exception, nevertheless these too should also be designed to be unobtrusive.
Low-cost affordability and reliability: When viewed from a cost versus life-saving benefit - the question of affordability translates to reliability. One aspect of that is low to no false positives (false alerts) and false negatives (missed alerts). Incompatibilities between the diagnosis of mRPMs and Physicians can also lead to a drastic drop in perceived value. Reliable also means it has to be always available. By reducing power consumption for mobile devices and speeding up recharging time, we decrease the downtime thus improving the reliability.
Let me now set the stage for you: Imagine trying to build a viable long-term safe mRPM network with a hodgepodge of largely unregulated market-driven mRPMs all sending data to a centralised server over the Internet. So what can go wrong, you ask? Well, plenty!

Let’s take a closer look:
Non-standard hardware aka Physical layer: The vast array of original equipment manufacturers using incompatible proprietary hardware makes integration, management and maintenance a nightmare. Over time, vendors will invariably go out of business and spare parts will become unavailable - but the patient and their needs will not - creating a nightmarish problem.
Out-of-date Application layer software: Once devices are deployed in the field, updating the software with bug fixes and new features becomes a challenge, especially for non-technical users. Good product design must make automatic updates reliable, seamless and painless with minimum downtime. The design should avoid bricking the system in case of malfunctioning updates, so as to make the device more reliable.
Network layer Security: IoMT modules are connected to the Internet making them potential targets for hackers. Sadly the low-cost, low-energy design often sacrifices security for functionality. Without a constantly up-to-date security system, IoMTs are exposed to hackers via the Internet. With minimal standardisation of the underlying operating system, rolling out a security patch, even if a fix should be made available, becomes impractical to test and roll out quickly and with high confidence of not bricking the unit.
By taking control of IoMT devices, perpetrators may jeopardize patients’ safety and privacy by way of data theft and corruption. Or worse still hijack control of the device for ransomware or to modify IoMT use and functionality.
Network security can be improved with a Zero-trust network security model, one in which communication among devices is controlled by strict access control and authentication to ensure traffic is between legitimate devices. Increased security can be achieved with better SSL/TLS (secure sockets layer and transport layer security) and authentication algorithms including 2-factor authentication (2FA), cloud-based authentication and blockchain-based decentralized authentication.
Centralized systems should enact strict firewall rules to deny traffic from all but trusted servers, deploy centralized certificate signing, activate intrusion detection systems,
Competing Networking Protocols for IoMT: Wireless Body Area Network WBAN is a new and evolving IEEE 802.15.6 international standard for low power, short range, and extremely reliable wireless communication within the surrounding area of the human body. In addition, apart from the ubiquitous WiFi standard (IEEE 802.11) but higher power and range means higher Rf and associated health risks. A more suited alternative is the Bluetooth Low Energy (BLE) standard (IEEE 802.15.1 that evolved from a broader Bluetooth standard 802.15) and ZigBee (IEEE 802.15.4). While no size fits all, it is important to know the power consumption and range of these when designing the device. Furthermore, since these devices all operate in the unregulated frequencies of 900MHz, 2.4GHz and 5GHz, devices that avoid the congested frequencies will benefit from increased reliability.

References
Halamka, J. (2023). The future belongs to remote patient monitoring. Mayo Clinic Platform. https://www.mayoclinicplatform.org/2023/02/27/the-future-belongs-to-remote-patient-monitoring/
Vaghasiya, J. V., Mayorga‐Martinez, C. C., & Pumera, M. (2023). Wearable sensors for telehealth based on emerging materials and nanoarchitectonics. Nature, 7(1). https://doi.org/10.1038/s41528-023-00261-4
Majumder, S., Mondal, T., & Deen, M. J. (2017). Wearable sensors for remote health monitoring. Sensors, 17(12), 130. https://doi.org/10.3390/s17010130






Thank you for drawing attention to the bigger picture and attention that must be paid to long term sustainability and reliability in this inevitable move towards remote healthcare.
ReplyDelete